RECESSED CHIN
A chin that sits behind where it should — from mild microgenia to severe Class II retrognathia. Honest breakdown of what the term actually means, how to assess your own from a photo, what causes it, and the real comparison of chin filler, genioplasty, and chin implants.
- →"Recessed chin" covers three different things: microgenia (small chin button, normal bite), retrogenia (chin specifically lacks projection), and retrognathia (whole mandible is set back). Different fixes for each.
- →Standard reference is the Ricketts E-line: chin should sit on the nose-tip-to-chin-tip line, with lower lip ~2mm behind it.
- →Chin filler is the highest-evidence non-surgical option. 9-18 months durability, 81% responder rate at 12 weeks (Restylane Defyne RCT 2024).
- →Genioplasty beats chin implants for moderate-to-severe cases (85% vs 66% soft-tissue translation, lower infection rate, can correct vertical not just horizontal).
- →Chin tucks don't fix recession. They retract the head, not the chin. Looksmax community confuses this.
Microgenia, Retrogenia, Retrognathia
Most pages on the internet call all three of these "recessed chin" — but they're clinically distinct conditions with different fixes. If you're going to consult a surgeon, knowing which one you have changes the conversation.
Underdeveloped chin button, normal bite
Your jaw position and bite are fine (Angle Class I). The mental protuberance — the bony button at the front of your chin — is just smaller than ideal. Forward projection is the problem; vertical height is usually fine. Fix: chin augmentation alone (filler, implant, or genioplasty).
Chin specifically set back from skeletal base
The chin's position relative to the rest of the face is recessed — your lips end up forward of the E-line because the pogonion (chin tip) is behind it. This is the category most people mean when they say "recessed chin." Fix: depending on severity, chin filler, sliding genioplasty, or implant.
Whole mandible is small / set back (Class II)
The entire lower jaw is underdeveloped or sits posteriorly relative to the upper jaw. Chin appears recessed because the whole jaw is. Often pairs with overbite, snoring risk, and potential sleep apnea. Fix: chin augmentation alone is insufficient. May need orthodontics, BSSO (bilateral sagittal split osteotomy), or combined orthognathic surgery.
Ideal Chin Projection
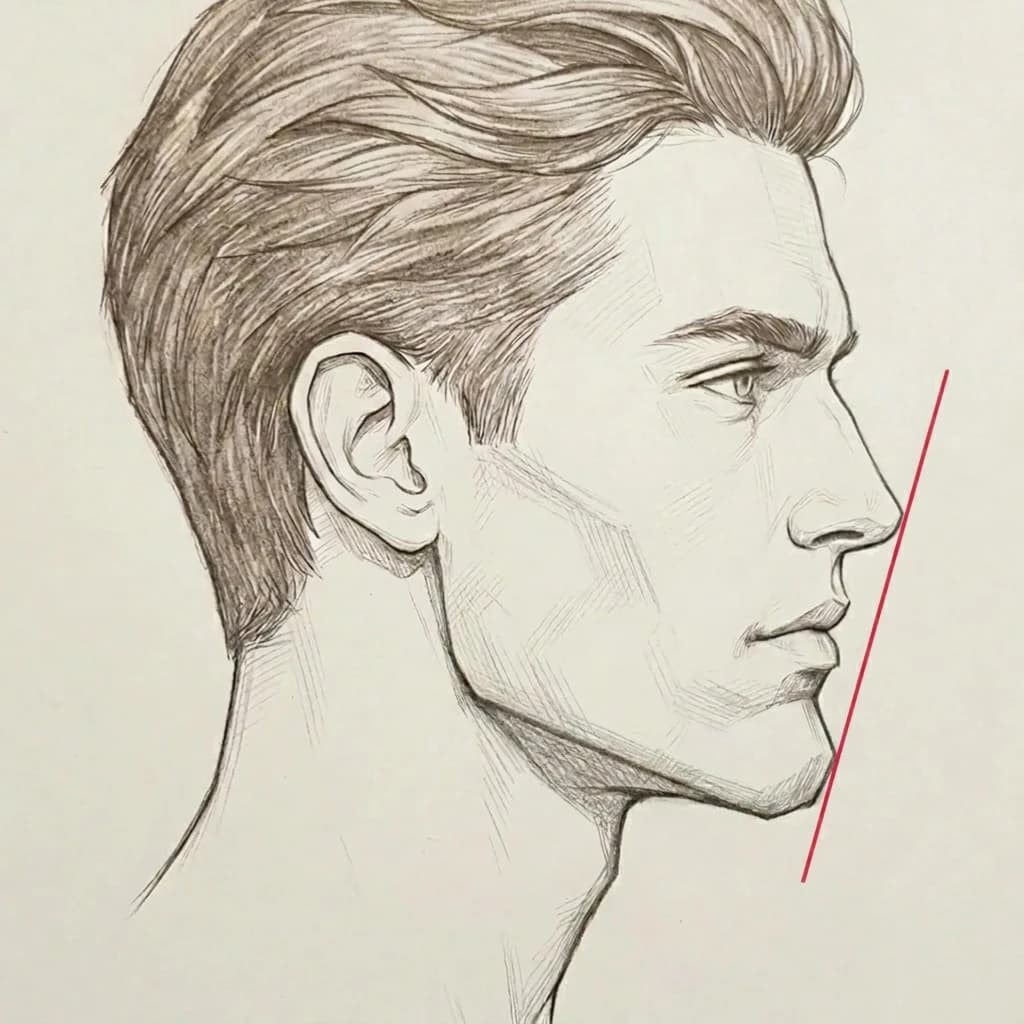
The E-line in red. Chin touches it; lips sit behind.
The Ricketts E-line standard
A line drawn from the most forward point of the nose (pronasale) to the most forward point of the chin (soft-tissue pogonion). On a balanced profile:
- Upper lip sits ~4mm behind the E-line
- Lower lip sits ~2mm behind the E-line
- Chin (pogonion) approaches or touches the E-line
Slightly forward / projecting chin preferred. Prominent lateral chin tubercles are a male sexual dimorphic trait. Attractiveness research consistently rewards the prognathic (correctly-projecting) male profile.
Asymmetry note: a 2022 attractiveness study (PMC8881019) found that -7.5mm chin deficiency drops attractiveness ratings by 2 Likert levels, while it takes +12.5mm of chin excess to drop ratings by the same amount. People tolerate chin excess far better than deficiency.
Softer contour, slight recessivity often preferred. Studies show women with less prominent chins score higher on lay-observer attractiveness ratings.
Practical implication: a chin that reads as "recessed" for a man may be perfectly normal or even desirable for a woman. Don't cross-apply standards.
Ethnic variation in E-line norms
Ricketts' original norms came from a Caucasian sample. African, East Asian, and South Asian populations have naturally more protrusive lip and chin profiles relative to the original baseline. If you're comparing your profile to the Ricketts standard, expect some natural offset based on ethnicity. The line is directionally useful, not universally applicable.
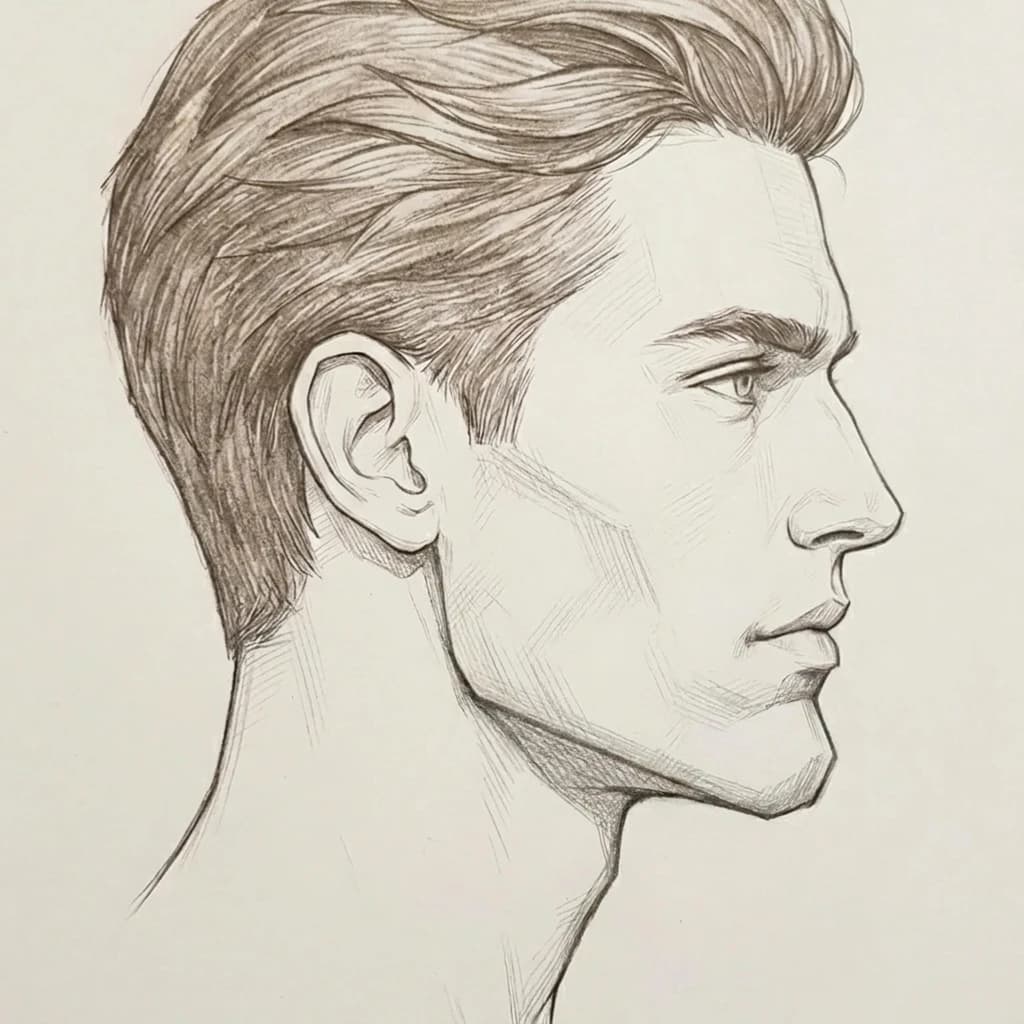
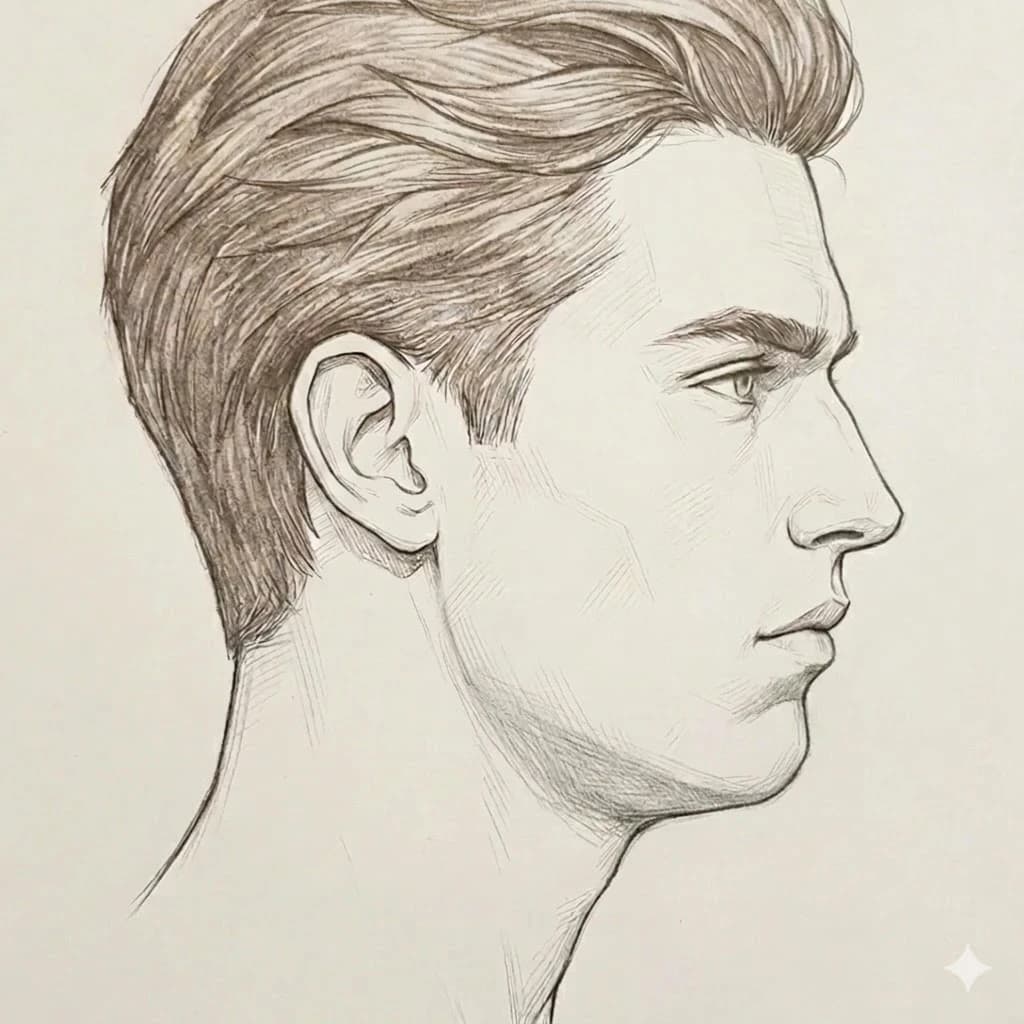
Chin Projection Across The Spectrum
Same character drawn three ways. Only the chin projection differs. Compare your own profile to find roughly where you sit.
Chin sits clearly forward of the lower lip, touching or slightly ahead of the Ricketts E-line. The masculine ideal — prominent lateral chin tubercles, forward-projecting pogonion.
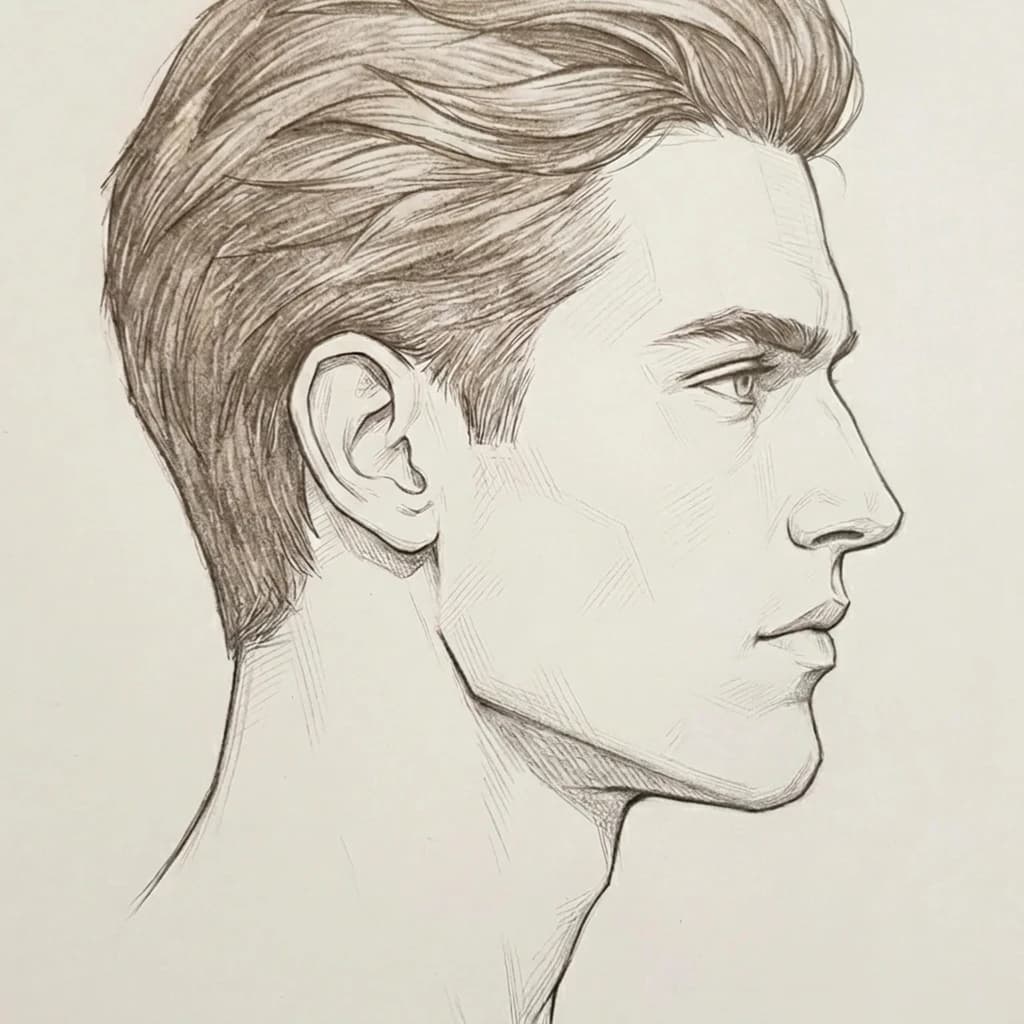
Chin roughly aligned with the lower lip, slight setback from the E-line. Population average — neither dominant nor weak. Most men land here.
Chin sits behind the lower lip and clearly behind the E-line. The chin slopes back into the neck without a clear chin point. Class II skeletal pattern.
Self-Assessment From A Profile Photo
Five steps. Free. Directional only — not a substitute for clinical evaluation.
Take a strict profile photo
Camera at eye level, perpendicular to your face. Neutral head — no chin lift, no chin tuck. Lips relaxed and closed. Phone roughly 3-5 feet away to minimize lens distortion.
Identify the two endpoints of the E-line
Pronasale: the most forward point of your nose tip. Soft-tissue Pogonion: the most forward point of your chin (the very tip in profile). Mentally draw a straight line connecting these two points — this is the Ricketts E-line.
Read where your lower lip and chin fall
Standard reference: upper lip ~4mm behind the line, lower lip ~2mm behind the line, chin essentially on the line. If your lower lip sits significantly ahead of the E-line, or your chin clearly sits behind it, your chin is recessed relative to the standard.
Apply sex and ethnicity context
Ricketts' norms were derived from a Caucasian sample. African, East Asian, and South Asian populations have naturally more protrusive lip/chin norms. Sex matters too: men ideally project slightly more forward than women. A 'recessed' chin by male standards may be perfectly normal for a woman.
Apply the honesty filter
Photo-based assessment is directional, not diagnostic. Lens distortion, head rotation, and beard mass all distort the read. Use the result to identify the category (clearly recessed / borderline / normal projection) — not to argue specific millimeters. Definitive measurement requires a lateral cephalometric X-ray.
Our free Jawline Test scores chin projection as one of 5 components. Same accuracy ceiling as manual photo assessment, less manual work.
What Causes A Recessed Chin?
Five real causes ranked by impact and evidence quality.
Genetic / skeletal pattern
well-establishedPrimary cause. Recessed chin tracks family lines closely — the underlying mandibular growth pattern and the size of the mental protuberance are both substantially heritable. This is the cause you can't change without surgery.
Class II skeletal pattern (retrognathia)
well-establishedWhen the entire mandible is underdeveloped or set back relative to the maxilla, the chin appears recessed because the whole jaw is. This is a structural pattern (not just a chin issue) and often pairs with overbite, snoring risk, and potential sleep apnea concerns. Chin augmentation alone doesn't fix Class II — the skeletal base needs addressing.
Childhood mouth breathing / adenoid facies
well-documentedA 2021 systematic review (PMC7944632) confirmed chronic mouth breathing in children causes posterior-inferior mandibular rotation, increased lower facial height, and a Class II tendency — producing what orthodontists call 'adenoid facies.' The effect is strongest during growth and stable post-growth. If you had chronic enlarged adenoids or nasal obstruction as a kid, this may be why.
Aging — bone resorption + soft tissue changes
establishedBone resorption in the mandibular symphysis with age, plus submental fat accumulation and skin laxity, can produce apparent chin recession in someone who didn't have it at 25. Tooth loss in the lower anterior region also drives alveolar bone loss that reduces apparent chin height and projection.
Tongue posture / mewing (the claim)
plausible in children, not in adultsBiologically plausible during childhood — tongue posture genuinely affects maxillary and mandibular development in growing kids. In adults: zero peer-reviewed RCT evidence for skeletal change. Myofunctional therapy (proper breathing, swallowing, tongue posture) has pediatric orthodontic evidence; the looksmax community's adult mewing claims do not.
Can You Fix It?
- →Chin filler (HA) — single highest-evidence option. 81% responder rate at 12 weeks per the 2024 Restylane Defyne RCT, 74% sustained at 48 weeks. Reversible with hyaluronidase.
- →Body fat reduction — for pseudo-recession from submental fullness. Real lever for people whose chin recession is partly optical.
- →Beard styling — legitimate optical extension of the visible chin line. Longer chin, shorter sides.
- →Posture work — reduces forward head posture and makes the lower face read better in photos. Doesn't advance the chin itself.
- →Sliding genioplasty — bone is cut, advanced, fixed with titanium plates. Gold standard for moderate-to-severe cases. Corrects all three axes.
- →Chin implant — silicone, Gore-Tex, or custom alloplastic implant placed on the existing bone. Less invasive but only addresses forward projection.
- →BSSO (orthognathic surgery) — for Class II retrognathia where the entire mandible is set back. Bigger surgery, requires orthodontic co-treatment. Often combined with genioplasty.
- →Mewing — no adult skeletal evidence. Don't expect bone change.
Genioplasty vs. Chin Implant
The two main surgical paths for chin advancement. Different best-fit patients, different complication profiles.
| Sliding Genioplasty | Chin Implant | |
|---|---|---|
| What it is | Bone cut, advanced, fixed with plates | Alloplastic implant on existing bone |
| Soft-tissue translation | ~85% (predictable) | ~66% (less predictable) |
| Axes corrected | All three (AP / vertical / lateral) | AP only (forward) |
| Infection rate | 0-5.3% | Up to 23.8% |
| Reoperation rate | Low | Up to 19% in some series |
| Patient satisfaction | VAS ~7.8/10 | Lower in head-to-head studies |
| Recovery | Slower (bone healing 6-8 weeks) | Faster (1-2 weeks soft tissue) |
| Best for | Moderate-severe cases, vertical or asymmetric deficiency | Mild Class I cases, faster recovery preference |
Bottom line: for moderate-to-severe recession, the data favors sliding genioplasty on every metric except invasiveness. For mild Class I microgenia in a patient who wants faster recovery, chin implants are reasonable. For Class II retrognathia (whole mandible set back), neither is sufficient — that needs BSSO / orthognathic surgery, sometimes combined with genioplasty.
Score Your Chin In 60 Seconds
Our free Jawline Test scores chin projection as one of 5 structural components — alongside gonial angle, jawline sharpness, mandibular width, and symmetry — and gives you an honest read of where you sit on the Chiseled-to-Recessed spectrum.
FAQ
What's the difference between microgenia, retrogenia, and retrognathia?+
All three are sometimes called 'recessed chin' but they're clinically distinct: (1) Microgenia: normal jaw position and bite, but the chin's bony button (mental protuberance) is underdeveloped — vertical height is fine, forward projection is the problem. (2) Retrogenia: the chin specifically lacks forward projection relative to the skeletal bases — lips end up in front of the E-line. (3) Retrognathia: the entire mandible is small and posteriorly positioned (Class II skeletal) — chin appears recessed because the whole jaw is. Microgenia can be fixed with chin augmentation alone. Retrognathia/Class II usually needs more — orthodontics, BSSO, or a combination.
Is my chin recessed?+
Use the Ricketts E-line: take a strict profile photo, mentally draw a line from your nose tip to your chin tip, and check where your lower lip and chin land. Standard: upper lip ~4mm behind the line, lower lip ~2mm behind, chin essentially on the line. If your lower lip clearly sits in front of the line or your chin is well behind it, you likely have at least mild recession. Important caveat: the standard E-line norms come from a Caucasian sample and don't account for the more protrusive lip/chin profiles common in African, East Asian, and South Asian populations — adjust for ethnicity. Sex also matters: men ideally project more forward, women slightly less.
What causes a recessed chin?+
Five main causes ranked by impact: (1) genetics — the dominant driver, runs in families, you inherit your skeletal growth pattern. (2) Class II skeletal pattern — the whole mandible is underdeveloped, chin recessed as a downstream effect. (3) Childhood mouth breathing — chronic nasal obstruction forces low tongue posture and posterior-inferior mandibular rotation, producing 'adenoid facies.' (4) Aging — bone resorption in the mandibular symphysis plus submental fat plus skin laxity. (5) Tongue posture during growth — the mewing claim has pediatric evidence but no adult evidence.
Can you fix a recessed chin without surgery?+
You can shift the appearance significantly but you cannot change the underlying bone position. Highest-evidence non-surgical lever: chin filler (hyaluronic acid). A 2024 RCT on Restylane Defyne for chin augmentation showed an 81% responder rate at 12 weeks, with 74% sustained at 48 weeks. Lasts 9-18 months. Other levers: body fat reduction (for pseudo-recession from submental fullness), beard styling (legitimate optical lever for men), and posture work. None of these change the bone — they change how it reads.
Do chin tucks help with a recessed chin?+
Important nuance: chin tucks RETRACT the head backward (correcting forward head posture) — they do NOT advance the chin. The looksmax community sometimes confuses this. Chin tucks help your jawline read better in photos by reducing forward head posture and submental neck-fat folding, but they do nothing to address the underlying chin projection. Don't expect to fix microgenia with posture work.
Genioplasty vs chin implant — which is better?+
Both work; they solve slightly different problems. Genioplasty (sliding genioplasty / osseous genioplasty) cuts and advances the chin bone, fixing it with titanium plates. Gold standard: 85% bony-to-soft-tissue translation, can correct all three axes (forward, vertical, side-to-side), patient satisfaction VAS ~7.8/10 in studies, very low infection rate (0-5.3%). Chin implants (silicone, Gore-Tex, or custom) sit on top of the bone — less invasive but only address the forward dimension and have a higher complication rate (infection up to 23.8%, reoperation up to 19% in some series). Genioplasty wins for moderate-to-severe cases and patients who need vertical adjustment. Implants win for mild cases and patients who want faster recovery. Neither is right for Class II skeletal patients — those need BSSO or orthognathic surgery first.
How long does chin filler last?+
9-18 months pooled across studies, with most patients seeing 12+ months from a single treatment with high-G' fillers like Restylane Defyne or Voluma. The 2024 RCT on Defyne for chin augmentation showed 81% responder rate at 12 weeks and 74% still responding at 48 weeks. Reversible with hyaluronidase if you don't like the result. Caveat: filler adds projection to your existing bone — it can't correct underlying Class II or severe microgenia, and at very high volumes the result starts looking artificial.
Does mewing fix a recessed chin?+
Honest answer: not in adults. Mewing has plausible biological mechanism for childhood and adolescent mandibular development, and myofunctional therapy is recognized in pediatric orthodontics. For adults whose bone is already fully formed: no peer-reviewed RCT evidence shows skeletal change from tongue posture training. The American Association of Orthodontists explicitly says no for adult structural change. Treat mewing as breathing/posture practice, not as a recessed chin fix.
Recessed chin in men vs. women — is there a difference?+
Yes, and most pages don't address this. Male attractiveness research consistently rewards a chin that projects slightly forward — prominent lateral chin tubercles are a male sexual dimorphic trait. Female attractiveness research shows a slightly more recessed / softer chin contour is often preferred. This means a chin that reads as 'recessed' for a man may be perfectly normal or even desirable for a woman. Don't apply male standards to female chins or vice versa.
Can a recessed chin cause health problems?+
It can. Severe retrognathia (whole-mandible recession, Class II skeletal) is associated with overbite issues, snoring, and obstructive sleep apnea — the airway behind the tongue gets smaller when the mandible sits further back. If your recession is significant and you snore heavily, wake up unrefreshed, or have other sleep symptoms, see a sleep doctor and an orthodontic / oral surgery consult. Mild microgenia (just an underdeveloped chin button on an otherwise normal jaw) is purely cosmetic.
Why is a small chin tolerated less than a big chin?+
A 2022 attractiveness study (PMC8881019) quantified this: a -7.5mm chin height reduction drops attractiveness ratings by 2 Likert levels, while it takes +12.5mm of chin excess to drop ratings by the same amount. People tolerate chin excess far better than deficiency. The explanation is evolutionary signaling — a strong forward chin is a marker of mandibular development and (in men) testosterone exposure during growth; deficiency reads as developmental softness. This is part of why even mild recession reads disproportionately negatively.
Sources
- Ricketts E-Line — original cephalometric reference — Standard reference line for chin/lip projection
- Microgenia clinical classification (Dr. Kirwan) — Microgenia / retrogenia / retrognathia distinction
- Influence of chin height on perceived attractiveness (PMC) — Chin excess vs. deficiency tolerance asymmetry (-7.5mm vs +12.5mm)
- Chin projection preferences by facial type and sex (PMC) — Sex and facial-type-specific projection preferences
- Mouth breathing and skeletal facial development — systematic review (PMC) — Childhood mouth breathing as cause of Class II tendency
- Implant vs. osseous genioplasty — systematic review (PMC) — Genioplasty vs. chin implant outcomes comparison
- HA filler chin augmentation RCT (Restylane Defyne, PubMed) — Chin filler responder rate and durability data
- Cleveland Clinic — Sliding genioplasty — Surgical procedure overview
- Cleveland Clinic — Retrognathia — Class II skeletal pattern overview
Related
- Jawline Test — score your jaw across 5 structural traits
- Gonial Angle — the angle at the corner of your jaw
- Chin Tucks — the daily exercise that sharpens the visible jawline
- Hunter Eyes Test — eye area structure read
- Canthal Tilt Test — measure your tilt in degrees
- Mogger Test — overall PSL classification
- What is mogged?
- What is looksmaxxing?