MIDFACE RATIO
The looksmaxxing metric for how compact the middle third of your face is. Honest breakdown of both community formulations, the 1.0-1.1 ideal range, photo self-measurement protocol, and what (if anything) you can do about it.
Upload a front-facing photo — AI measures your midface ratio in ~60 seconds.
Photo discarded immediately. No signup. No data stored.
- →Midface ratio = interpupillary distance ÷ pupil-to-lip distance. Higher = more compact midface = generally more attractive.
- →Ideal range: 1.0-1.1. Below 0.9 reads as long-faced. Above 1.3 starts looking unusually compact.
- →Long midface is mostly genetic + childhood mouth breathing. Vertical maxillary excess is the underlying skeletal pattern.
- →You can't change adult bone without surgery. Le Fort I osteotomy is the gold standard for impacting the maxilla and reducing midface height.
- →Mewing won't fix a long midface in adults. Plausible during growth, no evidence post-growth.
Two Definitions, One Concept
The looksmaxxing community uses "midface ratio" in two different ways. Most pages on the internet pick one without explaining the other. Both are valid; they measure related-but-distinct things.
Interpupillary distance ÷ pupil-to-lip distance
Take the horizontal distance between your pupils. Divide by the vertical distance from the pupil line down to the top of your upper lip (subnasale area). Higher ratio = more compact midface. This is the formulation most-cited on looksmax.org and the one used in community ratio-tier discussions. Ideal: 1.0-1.1.
Mid-third height ÷ lower-third height
The classical canon divides the face into three equal vertical thirds: trichion (hairline) → glabella (between brows), glabella → subnasale (bottom of nose), and subnasale → menton (chin). Equal thirds (1:1:1) is the textbook ideal. The midface ratio in this formulation is the mid-third compared to the lower-third — ideal is roughly 1:1.
Practical reconciliation: the community formula and the facial-thirds formula generally agree on what looks good (compact midface = attractive), but they aren't directly interchangeable. The rest of this page uses the dominant community formula (IPD ÷ pupil-to-lip), which is what most users encounter on looksmax forums and YouTube.
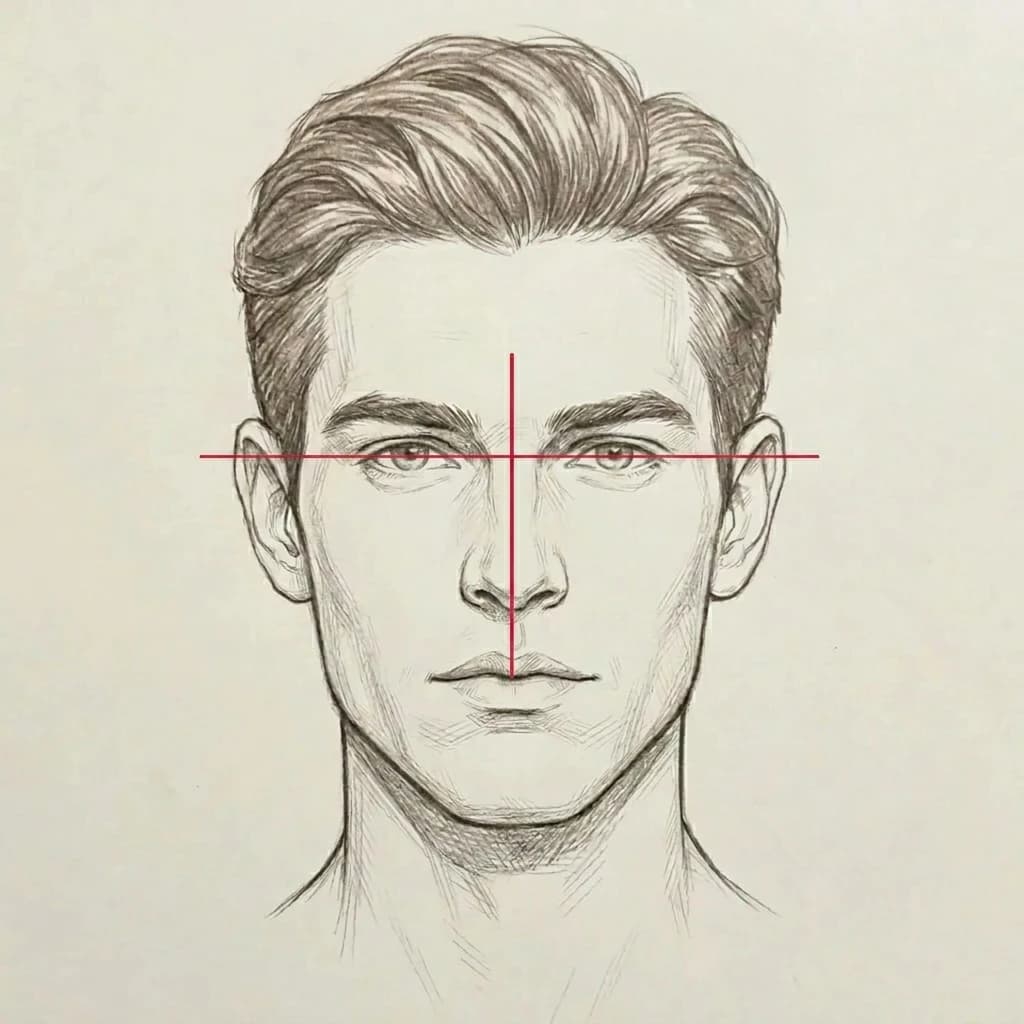
The two measurement lines: horizontal IPD + vertical pupil-to-lip.
How The Ratio Is Calculated
Two lines, one ratio. The horizontal red line shows the interpupillary distance (IPD) — pupil center to pupil center. The vertical red line shows the pupil-to-lip distance — from the IPD line down to the top of the upper lip.
Midface Ratio = IPD ÷ pupil-to-lip distance. Higher = more compact midface (features stacked closer together). Lower = longer midface (features spaced further apart vertically).
Midface Ratio Tiers
| Ratio | Tier | Visual Read |
|---|---|---|
| ≤ 0.85 | Very long midface | Often associated with vertical maxillary excess / long-face syndrome. |
| 0.86-0.94 | Long midface | Mid-third visibly longer than lower-third. Common in chronic mouth breathers. |
| 0.95-1.04 | Average | Population average. Neither dominant nor weak feature. |
| 1.05-1.15 | Compact / ideal | The visual sweet spot. Reads as harmonious and youthful. |
| 1.16-1.30 | Very compact | Stacked features. Generally attractive. |
| >1.30 | Extremely compact | Rare. Can start reading 'stacked' or unusual. |
Sex differences: generally minimal. The same ideal range applies to men and women. Female faces tolerate slightly longer midfaces without strong penalty in attractiveness research.
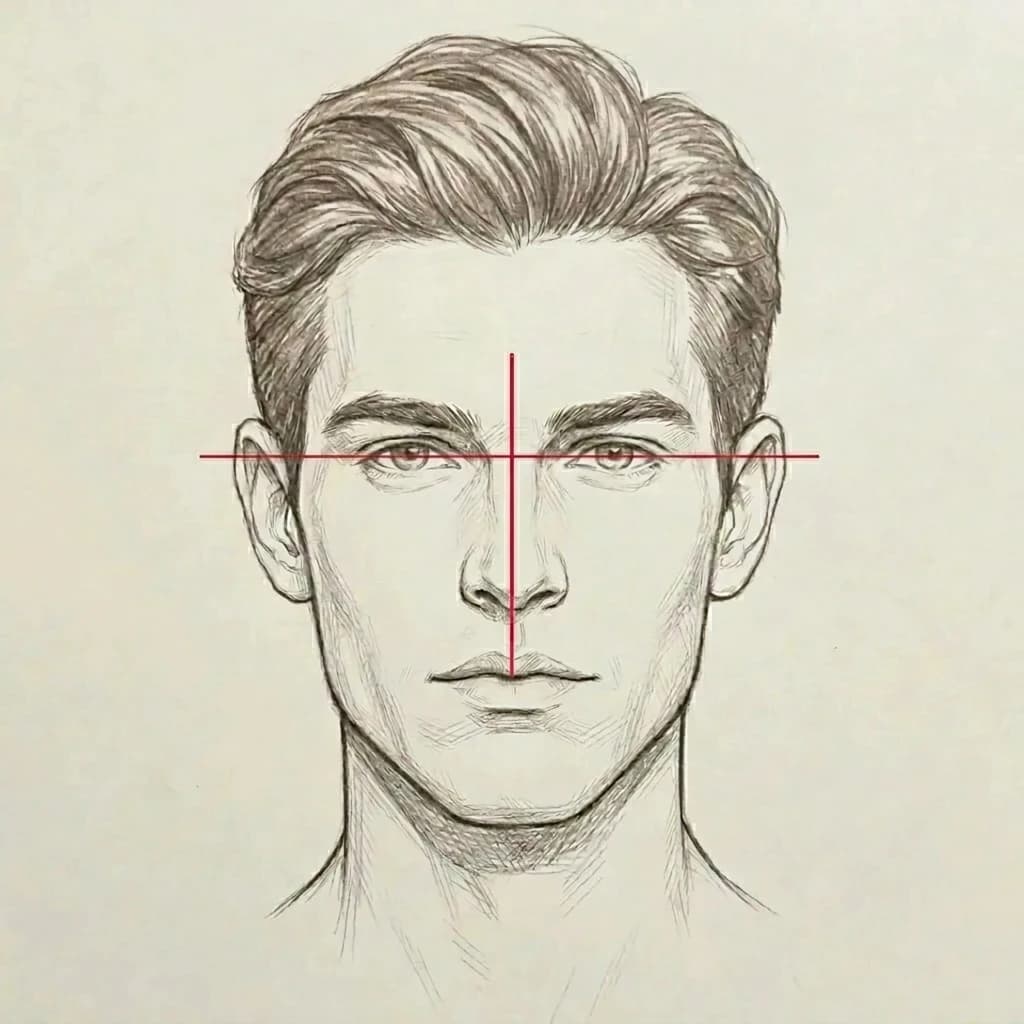
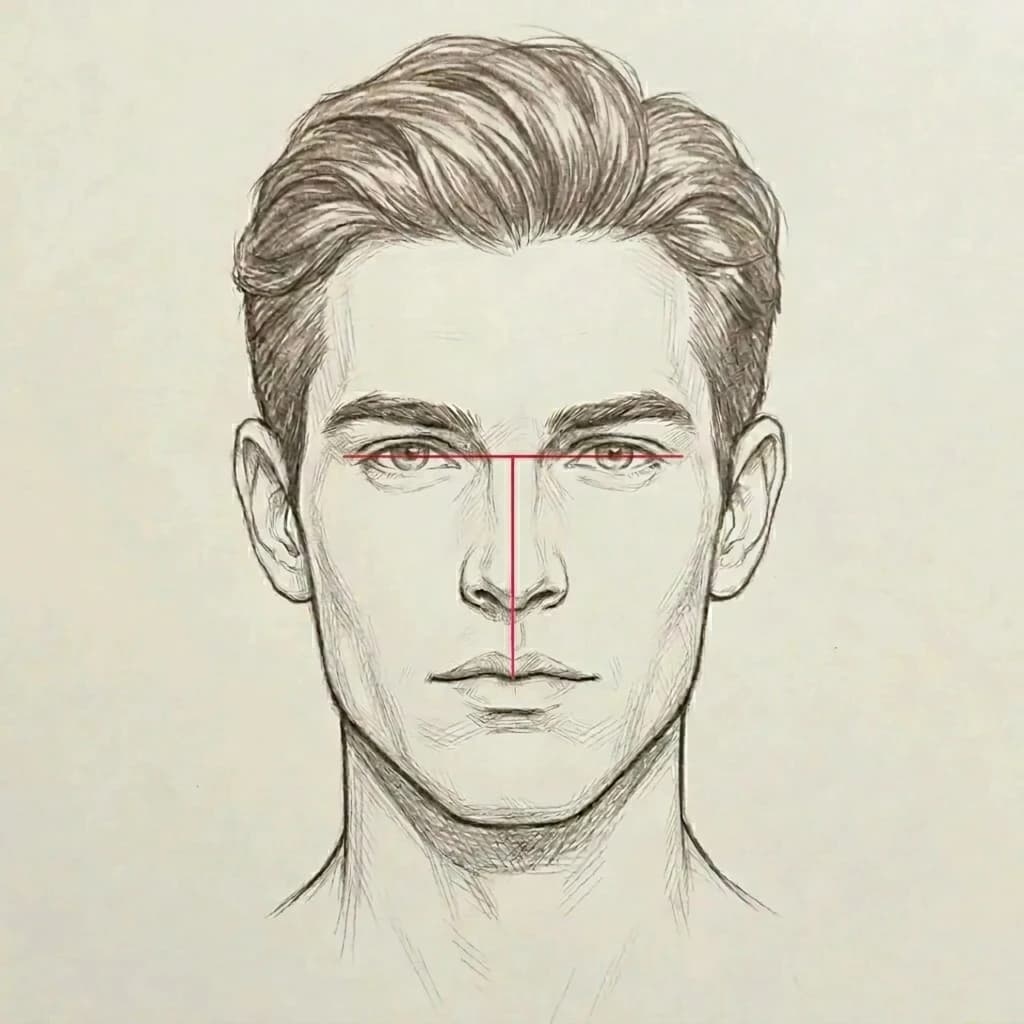
Midface Across The Spectrum
Same character drawn three ways. Only the midface proportions differ. Compare your own front-facing photo to find roughly where you sit.
Ratio < 0.9. Distance from eyes to upper lip stretches longer than the interpupillary distance. Often associated with vertical maxillary excess / long-face syndrome.
Ratio ≈ 1.0. Eyes-to-lip distance roughly equal to IPD. Population average — neither stacked nor stretched. Most men land here.
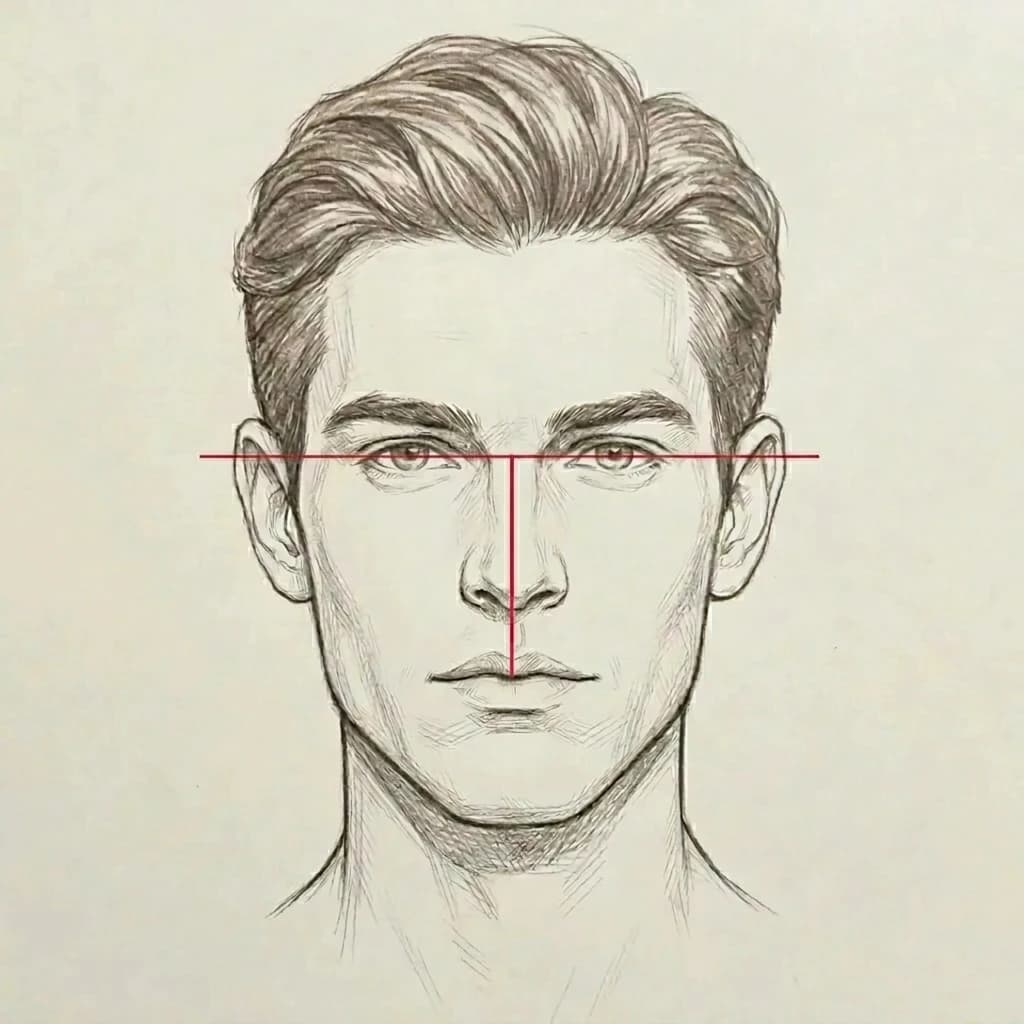
Ratio 1.0-1.1+. Features stacked closer together — short distance from eyes down to upper lip relative to IPD. The visual sweet spot — reads as harmonious and youthful.
How To Measure Your Own
Five steps. ~5 minutes. Free.
Take a strict front-facing photo
Camera at eye level, perpendicular to your face. Neutral expression. Lips relaxed, not pursed. Hair off the forehead. Phone roughly 3-5 feet away to minimize lens distortion. Eye-tragus line should be horizontal (no head tilt).
Identify the four landmarks
Pupil line (horizontal line through the center of both pupils). Subnasale (the point where the bottom of your nose meets the upper lip — sometimes called the nasal columella base). Glabella (the smooth area between your brows). Menton (the lowest point of your chin in profile, but visible in front view as the bottom of the chin shadow).
Measure two distances (community method)
Distance A: interpupillary distance (IPD) — straight horizontal distance between the centers of your pupils. Distance B: from the pupil line vertically down to the top of the upper lip (subnasale area). Midface Ratio = A ÷ B.
Read your result against the ideal band
1.0-1.1 = compact / ideal. 0.9-1.0 = average. Below 0.9 = long midface (mid-third stretches the face downward). Above 1.1 = very compact, generally reads attractive. Above 1.3 = unusually compact, can read 'stacked' or short.
Apply the honesty filter
Photo measurement carries ±3-5% error from lens distortion, head rotation, and lip position. Don't argue 0.02 differences — use the result for the category (long / average / compact / very compact), not exact ratios. Definitive measurement is from a cephalometric radiograph.
The midface is one piece. Run our free Jawline Test for the lower face (5 components) or the Mogger Test for the overall PSL classification.
What Causes A Long Midface?
Three causes ranked by impact.
1. Genetics / skeletal inheritance
dominantVertical maxillary excess and hyperdivergent skeletal patterns are heritable. The shape of the midface is largely set by the underlying bone, which is set by your early 20s. Most long midface cases have a clear family pattern.
2. Childhood mouth breathing / adenoid facies
well-documentedChronic nasal obstruction (often from enlarged adenoids) forces low tongue posture during a critical growth window. The maxilla doesn't get the lateral palatal force that drives forward and upward growth, so it grows down instead — lengthening the midface vertically. The mandible rotates posterior-inferiorly in response. Result: long-face syndrome, long midface, weak chin. Harvard Mass Eye and Ear documents the "mouth breather face" pathway clearly.
3. Maxillary hypoplasia (underdevelopment)
establishedUnderdevelopment of the upper jaw can produce a visually disproportionate midface even without vertical excess. Often part of broader skeletal Class III patterns. Treated surgically (Le Fort I advancement, or Le Fort II / III for more complex cases).
Can You Change It?
- →Hairstyle — a fringe or a hairstyle that lowers the apparent forehead boundary visually shortens the upper third, which shifts overall facial-thirds balance.
- →Brow shaping — fuller, slightly lower brows compress the apparent upper third.
- →Beard / stubble — adds visual mass to the lower third, balancing a long midface visually.
- →Mewing — for adults, no skeletal change. Maintain tongue posture for oral airway, don't expect midface change.
- →Le Fort I osteotomy — gold standard. Maxilla cut horizontally and impacted (moved upward). Reduces midface vertical height typically 5-10mm.
- →Le Fort II / III — for severe or syndromic midface hypoplasia. More invasive than Le Fort I.
- →Bimaxillary surgery — Le Fort I + BSSO together. Addresses both jaws when both are skeletally implicated.
- →Cheek / malar implants — don't change vertical height but add width and projection at the cheekbone, creating illusion of more compact midface.
Score The Rest Of Your Face
Midface is one piece. Our free tools cover the eye area (Hunter Eyes Test), the lower face (Jawline Test), and overall PSL classification (Mogger Test).
FAQ
What is the midface ratio?+
Midface ratio is a looksmaxxing-community metric for how compact the middle third of the face is. The dominant community formula is interpupillary distance (IPD) divided by the vertical distance from the pupil line down to the top of the upper lip. A higher ratio = a more compact midface. The classical orthodontic equivalent is the rule of facial thirds — the face should divide into roughly equal upper, mid, and lower thirds. Both formulations are addressed below.
What's the ideal midface ratio?+
Looksmax community consensus centers on 1.0-1.1 — interpupillary distance roughly equal to or slightly greater than pupil-to-lip distance. Below 0.9 reads as long-faced. Above 1.3 reads unusually compact. The ideal band 1.05-1.15 is the visual sweet spot. There's no strong sex difference in the cited norms — the same ideal range applies to men and women, though female faces tolerate slightly longer midfaces without strong penalty.
How do I measure my midface ratio from a photo?+
Take a strict front-facing photo at eye level, neutral expression. Measure (A) the horizontal distance between your pupil centers — your IPD. Measure (B) the vertical distance from the pupil line down to the top of your upper lip. Divide A by B. That's your midface ratio. Use a photo measurement app like Pixozone or Angle Meter 360 for precision, or the Mogged Jawline Test which scores related facial proportions automatically.
What's a long midface?+
A midface ratio below 0.9 — meaning the mid-third of your face (roughly eye line to bottom of nose) is longer than your lower-third (bottom of nose to chin). Visual effect: the face reads as 'long-faced,' droopy, or aged. The nose-to-lip distance appears excessive. Often associated with long-face syndrome (vertical maxillary excess), which is itself often associated with chronic childhood mouth breathing and adenoid facies. See our weak-jawline page for the broader long-face pattern.
What's a compact (short) midface?+
A midface ratio above 1.0 — the mid-third is shorter than the lower-third. Visual effect: features stack closer together, the face reads as more youthful and harmonious. Above 1.3 it can start to look unusually short. The compact midface is the look most associated with male attractiveness in looksmax discourse.
What causes a long midface?+
Three main causes: (1) genetics — vertical maxillary excess and hyperdivergent skeletal patterns are heritable. (2) Childhood mouth breathing — chronic nasal obstruction forces low tongue posture, which removes lateral palatal force and permits posterior-inferior mandibular rotation. The maxilla also grows downward rather than forward, lengthening the midface vertically. (3) Adenoid facies — the same mechanism as childhood mouth breathing, often triggered by chronically enlarged adenoids. Once skeletal growth is complete by the late teens / early 20s, the pattern is essentially fixed.
Can I fix my midface ratio without surgery?+
For adults: not meaningfully. The skeletal pattern is fixed by your early 20s. What you can change is visual perception — hairstyle that lowers the apparent forehead boundary, brow shaping that compresses the apparent upper third, and beard or stubble at the lower face that adds visual weight to the lower-third. These shift the visual balance modestly without changing any underlying anatomy.
Does mewing fix a long midface?+
In adults, no. The mewing claim is that proper tongue posture (tongue against the palate, applying upward pressure) drives forward and upward maxillary development. Biologically plausible during childhood and adolescent skeletal growth. In adults: zero peer-reviewed evidence for skeletal change, sutures are fused, the maxilla doesn't move. Do mewing for tongue posture and oral airway benefits if you want — don't expect midface change.
What surgery fixes a long midface?+
Le Fort I osteotomy is the gold standard. The maxilla is cut horizontally and impacted (moved upward), reducing midface vertical height by typically 5-10mm. For more severe or syndromic cases: Le Fort II / III, or bimaxillary surgery (Le Fort I + BSSO) addresses both jaws. SARPE (surgically assisted rapid palatal expansion) addresses width but not vertical. Cheek/malar implants don't change vertical height but can create the illusion of more compact midface by adding width and projection.
Long midface vs weak jawline — what's the difference?+
They often appear together but they're separate measurements. Long midface refers specifically to the proportion of the middle face third (eye line to nose) being too tall relative to the lower third. Weak jawline refers to the lower face — gonial angle, jawline sharpness, chin projection, mandibular width. Many people with vertical maxillary excess have BOTH a long midface AND a weak chin/jaw because the mandible rotates posterior-inferiorly when the maxilla grows down. See our weak-jawline page for the lower-face deep-dive.
Sources
- Mommaerts MY (2016) — Ideal male jaw angle survey — Reference for related lower-face proportion norms
- Mass Eye and Ear / Harvard — Mouth Breather Face — Childhood mouth breathing → vertical facial growth pattern
- Long face syndrome — Instituto Maxilofacial — Vertical maxillary excess clinical overview
- Le Fort I osteotomy — PMC — Surgical procedure for midface impaction
- Evaluation of facial beauty — PMC — Classical facial-thirds canon and aesthetic proportions
- AAO — Does mewing actually reshape your jaw? — Authoritative no-evidence-in-adults statement on mewing
Related
- Weak Jawline — the lower-face composite
- Recessed Chin — chin projection deep-dive
- Gonial Angle — the angle at the corner of your jaw
- Chin Tucks — the daily exercise for jaw definition
- Jawline Test — score your jaw across 5 traits
- Hunter Eyes Test — eye area structure
- Canthal Tilt Test
- Methodology — how we score
- What is mogged?
- What is looksmaxxing?